
Outlive Part 3: Testing, Exercise, and Nutrition
Homework time

This is part three of my summary of Peter Attia’s Outlive. Here’s part one and part two. It’s too long to fit in one email, so make sure you click through to read the full thing!
Finally, the good stuff: ACTION ITEMS.
Outlive offers a wealth of information on improving longevity, but to keep things manageable, we'll focus on three key areas: testing, exercise, and nutrition; along with liberal use of footnotes so we can make it through everything without getting too bogged down.
So lock in and let’s get down to business.
Testing
Before we dive into specific tests, let's address an important caveat: reference ranges. While most lab results include “normal” ranges for each metric, these ranges can be misleading. Here's why:
Reference ranges are based on general population distributions.
As society has become less healthy overall, these ranges have shifted.1
What's considered “normal” may not be optimal for longevity.
Therefore, it's crucial to look beyond whether your results fall within the provided ranges. This also seems like a good place to once again say: I am not a doctor, none of this is medical advice, you should do your own research, etc. Always consult with a healthcare professional to interpret your results in the context of your overall health and longevity goals.
The top five tests
The first thing you run into when you start looking at testing is that it’s an acronym soup of a million tests you can take, most which aren’t immediately obvious what they’re even testing. Outlive doesn’t prioritize the top tests (another example of the overwhelming amount of information in the book), but Attia has talked about them elsewhere, and his top five are:
Lipoprotein (a) or Lp(a) - Lp(a) is an indicator of your personal predisposition toward heart disease. It doesn’t change, so you only need to check it once in your lifetime. If it’s elevated, then you need to pay extra attention to your ApoB levels and all the heart disease stuff we talked about earlier. If it’s <14 mg/dL you don’t get a free pass, you just have a “normal” amount of inherent risk.
ApoB - We talked about this in part two—this is the preferred way to gauge cardiovascular risk instead of just looking at “bad cholesterol”. ApoB will measure the amount of cardiovascular disease causing particles in your blood. Here’s an example of where reference ranges can be misleading. The test I took said my result of an ApoB of 95 mg/dL was in the normal range, so there was no need to worry, and it does appear to be at about the 50th percentile. But Attia advocates for an optimal range of <65 mg/dL, implying I still have a lot of room to improve.2
Oral glucose tolerance test (OGTT) - OGTT measures your insulin response and it appears to involve drinking an absolutely disgusting pure-glucose drink, and then waiting and drawing blood every 30 minutes to check your insulin response over time. If your body can get your blood glucose down to <140 mg/dL after two hours, then you’re normal. If it’s elevated still, that is bad. I can’t speak to this test because I haven’t done it, and it’s not clear if Attia recommends doing this even if you are otherwise young and healthy (he mentions it only once in all of Outlive). You can also get at some of the same data via a continuous glucose monitor, and the HbA1c test, even if OGTT remains the gold standard for assessing pre-diabetes.
Alanine transaminase (ALT) - ALT assesses liver health by checking if the ALT enzyme is leaking into the blood. ALT increases when your liver stores fat, which is one sign of metabolic dysfunction. This is commonly included in blood panels. Labcorp says <33 IU/L for women and <45 IU/L is normal, but "the American College of Gastroenterology recently revised it’s guidelines to recommend clinical evaluation for liver disease in men with ALT >33 and women >25. Attia unsurprisingly is even more aggressive, targeting <30 for men, and <19 for women.
APOE genotype - The APOE genotype determines an increased risk in developing Alzhemier’s disease risk. It’s one of the few tools we have to detect neurodegenerative diseases. This test is also a one-time thing. I can understand why Attia prioritizes this, but it seems like many of the things you want to do to decrease AD risk (like sleeping well, strength training, eating healthily) are things you want to be doing anyway to fight the other four horsemen, so I’m not sure how critical it is. At the very least, it seems similar to the Lp(a) test in that if you are at higher risk, you should take the recommendations a bit more seriously.
How to get tested
You have a few options to obtain the above tests:
Ask your doctor and get referred to a lab
This is easiest if you have easy access to your doctor, but they may be unwilling to order every test you want.
Roll your own directly with Quest Diagnostics (e.g., you can order this one, as well as a la carte) or Labcorp or go through something like Own Your Labs
This lets you bypass your doctor and just get the tests you want, but it can be daunting as no one makes it very easy to figure out what the hell you’re doing, and not every test seems to be available to the public, even if doctors can order them.
Use a third party (non-insurance based) service like Inside Tracker or Function Health
This is the most expensive option, but they handle a lot of logistics for you and provide nice UX for reviewing the results. These services all tend to use Quest or Labcorp for their blood draws and labwork, so you’re paying a premium on top. The downside for some is they try to upsell you into subscription plans or other related health tracking services. I haven’t tried either of them, but if you can afford it I’d probably just go with this for the convenience if my doctor was unwilling to order for me.
Other useful tests
Continuous glucose monitor (CGM) - CGMs are devices historically used by diabetics to monitor their blood glucose, but even if you aren't diabetic you can get one to wear to easily monitor your blood glucose from your phone.
Getting one requires a prescription for some crazy reason, but once you have one, you can get them for pretty cheap—the Freestyle Libre sensors cost up to $75 for two. They're painless and easy to put on, last for two weeks, and sync to your phone. The manufacturer, Abbott, seems to offer a free trial here. (Update: Apparently the FDA approved the first CGM for over the counter purchase without prescription earlier this year. It’s only for a specific model from Dexcom, but this hopefully means that they’ll all be available OTC soon. Thanks, Prabhu for the tip!)

CGMs sit on the back of your arm like this, are waterproof, and look really cool. You want to a) experiment to see what foods spike your glucose (e.g., for me a banana was surprisingly bad) because everyone is different, and b) see how the timing and order of what you eat affects your glucose response. The goal is to reduce the spikiness of our insulin response. For example, by first eating some protein and complex carbs (like beans), and then waiting ten minutes before eating dessert, I found my blood glucose is much less likely to spike as high. But waiting much longer to have dessert reduced the positive effect of the beans.
Stress and lack of sleep also impair your body's ability to dispose of glucose. If you're under a lot of psychological stress, the CGM may be a wakeup call to quit your job.
Attia targets 100 mg/dL avg glucose or lower, with std dev of less than 15 mg/dL. This is, to no one’s surprise at this point, extremely aggressive!
Cancer screening
As discussed in part two, the best tool we have to fight cancer is to screen early and often. This is why Attia recommends average risk individuals getting a colonoscopy starting at 40, instead of at 45, and repeating every 2-3 years depending on the findings.3
Two or three years might seem like a very short window of time to repeat such an involved procedure, but colon cancer has been documented to appear within the span of as little as six months to two years after a normal colonoscopy.
Strangely I don’t think he mentions any other specific screening outside colonoscopies in Outlive. Regardless, I guess one takeaway is do not skip any routine screening!
DEXA scan - A DEXA scan measures your bone density, but also can accurately measure the amount of fat you have, and importantly where it is located. Contrary to most body fat % measurements that attempt to use electrical signals, the DEXA scan uses x-rays to tell how much lean mass, fat, and bone you have in each part of your body. It can tell you how much visceral fat you have, which is the bigger worry, as opposed only total fat. I did mine at Dexafit, but just search for DEXA scans in your area to do one. You can do this once a year to track your visceral fat and bone density longitudinally.

You just lie down clothed on the scanning bed for about 5-10 minutes and you’re done!


Exercise
Now that we've covered testing, let's move on to the cornerstone of longevity: exercise. If there's one key takeaway from Outlive, it's this: EXERCISE IS THE MOST EFFECTIVE TOOL WE HAVE FOR LONGEVITY. While the tests we discussed are important, they serve little purpose if not paired with a solid exercise routine.
Attia recommends a balanced approach to exercise:
50% cardio, further divided into:
80% Zone 2 training (moderate intensity)
20% Zone 5 training (high intensity)
50% strength training
This approach addresses a common question: “Is strength training or cardio more important?” Attia’s answer should surprise no one—all of the above.
Let's break down each component:
Cardio
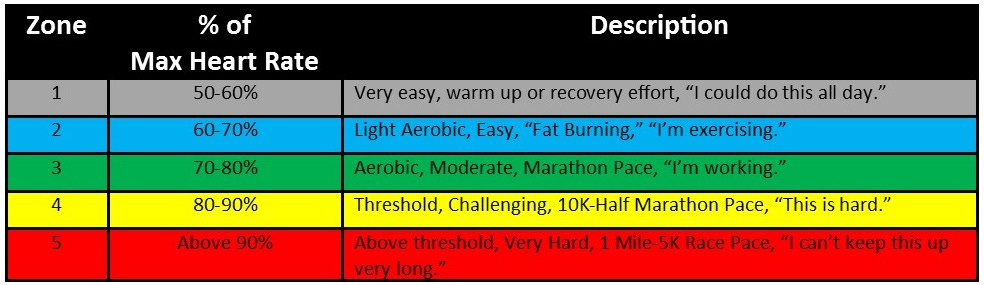
Cardio is split up by heart rate into different “zones”. Lower zones are lower heart rates. Lower zones burn fat (by calling on fat stores for energy), while higher zones use glucose for fuel.
Zone 2
Working in zone 2 burns fat, and improves the efficiency of our body’s ability to use fat as fuel. It's the most important exercise we can do to fight metabolic syndrome.4 The goal is 3 hours a week, or four 45-minute sessions for most people to see a benefit, but you probably can’t overdo it.
There are lots of different ways to measure whether your heart rate is in zone 2, but one easy heuristic is that you can talk in full sentences, but just barely. Another way is to target ~60-70% of your peak heart rate. As you practice, it should get easier, and you should expect to need to bump up your target over time.5
Zone 2 is not so taxing that you can't multitask, so you can use the time to listen to podcasts, watch videos, etc. I bought a cheap walking treadmill for my standing desk and use it while playing certain games or watching YouTube, etc. The key is to find a way to fit it into your lifestyle that works for you.

This seems like the wrong attire for zone 2 but you get the idea. (source)
Zone 5
In contrast to the relatively chill endurance training of zone 2, zone 5 is intense. Working in zone 5 improves VO2 max, or the maximum rate a person can utilize oxygen. VO2 max is expressed as the volume of oxygen you can use, per kg of bodyweight, per minute. An average 45yr old male will have a VO2 max of around 40 ml/kg/min. An unfit person in 30-40s might only score in the high 20s.
VO2 max can always be improved by training, no matter how old you are. Zone 5 training is much harder than zone 2, but the good news is you do not need to do it as often. 1-2 per week is enough. Attia claims it may be the single most powerful marker for longevity.6
Do cardio (bike, run, row, etc) for 4 minutes at the maximum pace you sustain for those four minutes (very hard, but not an all out sprint), then ride/jog/etc at an easy pace for 4 minutes of recovery so your heart rate drops back down to <100 bpm. Do this 4-6 times, and cool down.7 You don’t have to exactly follow this prescription—even just training zone 2 will also help improve your VO2 max. If you can fit in some occasional high-intensity cardio, you’re on your way.

Strength
Muscle mass and strength matter (unsurprisingly), especially as you age. Having more muscle mass protects you from plenty of things, but most importantly is correlated with a lower risk of falling, which is a leading cause of death and disability in the elderly.
It is never too late to start—Attia's mom started at 67! There are lots of studies showing strength training can improve mobility and physical function of all types of people, including those who are already elderly and frail. If you are older and unsure where to start, check out this specific podcast episode on exercise for aging people, or see this footnote for some quick notes to send to your parents.8 Attia aims to lift heavy weights in some form 3-5x/week. (He does a LOT of things 3-5x a week).
There are a few key movements that map to real-world activities that are useful to train, versus just having enormous biceps (though don’t let me stop you if that’s your goal, Daniel):
Pulling—can you carry groceries, lift heavy objects when you are old? All the typical pulling strength movements are good: lat pulldowns, rows, etc.
Hip hinge—can you get out of a chair without difficulty? You need to be careful of spinal injury with these, so you want to build up slowly, starting with things like single leg step-ups, and split stance Romanian deadlifts, all starting without weights.
Grip strength—can you hold onto railings to avoid falls, or open jars? Hands are our primary interface to the world, and grip strength strongly predicts how likely you are to live.9 If you spend time lifting barbells and dumbbells you will naturally build this. In addition you can perform the farmer's carry.

#goals (source) Attia’s goal is half our body weight in each hand (so full body weight total!) while walking for 1min for males, and 75% of body weight for females. This is very hard!
The dead hang is also a good test as a way to measure improvement.
For all of these exercises, don't forget the eccentric part of the movement (the release of the muscle after contracting. We tend to focus on the concentric portion such as when we are bringing the dumbbell up in a bicep curl, but ability to slowly release your muscle while holding a weight is valuable especially for the elderly because that's how we slow ourselves from a fall. If we grab onto to a railing to catch ourselves, it's our eccentric strength that reduces the impact.

Stability
Pushing yourself without adequate stability almost inevitably leads to injury. Your body is very good at compensating via "cheats". Attia likes to start with stability before adding any sort of strength training, including some of the assessments like dead hangs and single leg step-ups.
Attia spends 1 hour 1-2x/week doing dedicated stability training, with 10-15 min per day on other days, but mostly it's folded into every day training. If we're 80/20ing this, we can probably get away with just making sure we do it as part of our other training. Split-leg deadlifts, lunges, doing curls while standing on each leg, etc. Add in some core exercises, and you're good to go.
There's a whole section on how to breathe properly here that I will not go over, among other things like toe yoga.
There’s a lot of detail here, but just remember the goal of 50/50 strength/cardio, and 80/20 zone2/zone5. The rest is all further optimization that you can tailor to things you enjoy and your specific needs. Just start doing something!
Nutrition
When it comes to nutrition, it's important to recognize that there's no one-size-fits-all approach.10 Unlike exercise, which has more universal principles, nutrition needs vary significantly from person to person. The bloodwork and tests we discussed earlier can help determine your specific nutritional needs.
To simplify this complex topic, consider these key questions:
Are you under or overnourished?
Are you under or adequately muscled?
Are you metabolically healthy?
Most people in modern society fall into the category of being overnourished (consuming too many calories relative to energy expenditure) and undermuscled (insufficient exercise and/or protein intake). This combination often correlates with poor metabolic health.
With this context in mind, let's explore some general nutritional guidelines broken down by macronutrient type across the three types: carbs, protein, and fat. (Technically there are four—alcohol is it’s own category but unlike the first three, it’s nutritionally void and you don’t need it to survive.)
Carbs
The more refined the carbs (like white bread, regular pasta), the faster and higher the glucose spike. The more fiber or the less processed (like beans), the lesser the impact.
Attia targets more than 50g of fiber/day. Rice and oatmeal are surprisingly spiky, despite not being refined. Brown rice is only barely better than white rice (for glycemic-ness), though you should test and see for yourself on a CGM.
Non-starchy vegetables (spinach, broccoli) have no effect. Eat as much as you want.
High protein and fat have no effect on glucose.
Everyone knows soda is bad for you, but fruit juice is just as bad for glucose spikes. If you're drinking fruit juice in lieu of Dr Pepper, don't bother. Diet soda does not spike glucose.
Protein
Protein is the only macronutrient that is essential to our goals—there's no practical requirement for carbs or fats (assuming you are eating enough to survive, which is not hard), but you absolutely can be lacking enough protein.
The US RDA recommended amount is 0.8 g/kg which is baseline but not good. Studies show elderly people consuming that much and losing muscle mass!
Attia targets 1.6 g/kg/day as the minimum. Data suggests with normal kidney function, 2.2 g/kg/day is a good place to start.
Most people do not need to worry about overconsuming. The safe upper limit is 3.7 g/kg/day which would require a LOT of work to do. It is practically impossible to do this by accident.11
Fat
Fat gets a bad rap, but you need fat. It's a very efficient fuel, and also a building block of many hormones and cell membranes. Dietary fat also tends to leave you feeling fuller than many types of carbs, especially when combined with protein, which helps combat overeating.
There are three types of fat: saturated fatty acids (SFA), monunsaturated fatty acids (MUFA), and polyunsaturated fatty acids (PUFA). Within PUFA there are omega-3 variants, which can be subdivided into marine sources (EPA, DHA) like salmon, and nonmarine (ALA) sources like nuts/flaxseed. Then there are omega-6 variants.
Remember that most dietary cholesterol gets passed through your body, so it’s less about the amount of fat versus shifting the fat profile:
Attia advises to roughly try to get fat from 50% MUFA sources, reduce SFA to 15-20% and make the rest up with PUFA.
In practice this means: olive oil, avocados, nuts (MUFA) > butter, lard (SFA). If you take away one thing on fats, it should be to lower saturated fat consumption.
Reduce omega-6 rich oils like soybean, corn, sunflower oils.
Increase omega-3 marine oils via salmon and anchovies.
You need to monitor a lipid panel (apoB, cholesterol, etc) to track how changes in your fat composition affect your overall metrics. It does not work for everyone, so you must re-check.
None of this should be that surprising, and it’s nice to know that there is not one diet to rule them all. The guidelines are pretty simple: don’t eat too many or too few calories. Consume sufficient protein and essential fats (and cut down on saturated fats). Make sure you have the vitamins and minerals needed.
Coda
If you’ve made it all the way through this interminably long summary, I hope you’ve found it useful. I now understand why the summary for the book was fifteen pages long.
In compiling all of this, I have gone back and forth between “this guy is a madman who can not possibly have time for anything else” and “well at least he’s giving you all the context out there so you can decide for yourself”.
Attia can be polarizing, as this New Yorker piece attests:
Too often, conversations about life extension devolve into unhelpful abstractions and untestable speculation; one appeal of Attia’s advice is that it’s so tangible. Critics can paint his counsel as blindingly obvious or needlessly complex—but he has, at least, inspired large audiences to imagine what a better approach to aging could look like. “There is actually no such thing as atheism,” David Foster Wallace once said. “The only choice we get is what to worship.” In a society that chases money, power, fame, and beauty, there are worse gods than longevity.
Reading the tome that is Outlive, you get the sense that you are destined for failure unless you have insane levels of execution and willpower to do everything Attia suggests.
But as I’ve hopefully made clear, the value of Outlive is as a framework. You don’t have to do it all—perfect is the enemy of good. We aren’t aiming for perfect, we’re aiming for improvement so we can live longer, healthier lives.
I enjoyed Outlive because Attia’s obsession with longevity wasn’t just about extending lifespan, but about making your years enjoyable. In the end how you spend your time on this planet is the ultimate long game. Why not make it a game worth playing?
Thanks to Andrew Stevenson for reading drafts of this post.
For example, the average American adult male weighted 173 pounds in the late 1970s. Now the average American man is nearly 200 pounds.
Attia talks some more about ApoB in this four hour long interview (I told you he was verbose). ApoB is causally linked to Atherosclerotic Cardiovascular Disease (ASCVD)— when you have causal things that cause disease, you eliminate them. This is why he compares it to smoking. Because smoking is causal, so we tell you to stop, even before you have reached some threshold.
How low is “low enough”? He thinks that if your ApoB was <30 mg/dL, you literally couldn’t get ASCVD. Most people can’t get that low without drugs. But your current ApoB value is only part of the story: if you’ve never exceeded 60, that’s very different from starting at 120 and now being <60. We want to minimize the area under the curve, similar to how we measure “pack years” in smoking. An ApoB of 60 mg/dL is the 5th percentile.
Anything that contributes to insulin resistance is bad for ApoB. Higher triglycerides is worse. You want to work on lowering triglycerides, as they are an enormous proxy for insulin sensitivity. Cutting back on refined carbs is the most effective way to lower triglycerides. I know, I love ramen too. 😩
Attia includes some additional guidance on colonoscopies:
Before you get your first colonoscopy, there are [a] few things you can do that may improve your risk-to-benefit ratio. You should ask what your endoscopist’s adenoma detection rate (ADR) is. The ADR is the proportion of individuals undergoing a colonoscopy who have one or more adenomas (or colon polyps) detected. The benchmarks for ADR are greater than 30% in men and greater than 20% in women. You should also ask your endoscopist how many perforations he or she has caused, specifically, as well as any other serious complications, like major intestinal bleeding episodes (in a routine screening setting). Another question you should ask is what is your endoscopist’s withdrawal time, defined as the amount of time spent viewing as the colonoscope is withdrawn during a colonoscopy. A longer withdrawal time suggests a more thorough inspection. A 6-minute withdrawal time is currently the standard of care.
Mitochondria, the powerhouse of the cell, can use glucose and/or fat to create energy. Working at lower intensity (like zone 2) burns fat, while higher intensity loads draw on glucose. The healthier and more efficient your mitochondria are, the greater the ability to use fat, which is the most efficient and abundant fuel. We want to maximize our mitochondria’s ability to use fat because it helps control fat accumulation and spillover, and the best way to improve their efficiency is to just repeatedly use them to burn fat, hence training in zone 2.
It turns out there are lots of competing ways to estimate zone 2, and even different models can have five vs six vs seven different zones. If you look up zone 2 training online, you will find a confusing array of calculations that all spit out different answers. What matters is “going at a speed slow enough that one can still maintain a conversation but fast enough that the conversation might be a little strained.”
His explanation comes via a comparison: we know that smoking causes a 40% greater risk of all-cause mortality (the risk of dying at any moment) vs non-smoking. One study found that someone with below-average (25-50th percentile) VO2 max for their age/sex is at double the risk of all-cause mortality vs some one in the top quartile (75-97.6th percentile). It’s a little weird to compare these two since smoking is an action you can take, whereas low VO2 max is more likely a symptom of being generally unhealthy. There seems to be a high correlation of high VO2 max and longevity, but it’s not clear how much of that is just correlation. I find that it’s still a useful metric to at least track and see how you’re doing on relative fitness and health as you age.
Training VO2 max is a bit different from high intensity interval training (HIIT)—intervals there are ~30s there or less; for VO2 max you want 3-8min intervals (at less intensity). If you know your FTP wattage, target 120% of that for 3 minute intervals, and 106% of it for 8 minute intervals.
75% through the interval you should be at 50% of your pain. First min you don’t notice, 2nd minute you wonder if you should push harder, 3rd minute it’s hard, and 4th minute you’re dying. Fun!
From Exercise for Aging People:
Exercise variability and quality of movement are more important than volume, load, and intensity because you are much more prone to injury than when you are young.
Zone 2 output, VO2 max, and strength can all be improved at any age.
Cardio
Aim for a habit of doing something active daily (this can be walking!); move to very light weight on back (e.g., 20 lbs).
Need to build aerobic base (zone 2) first, before any kind of VO2 max. Target a heart rate of 180 - age - 10 if you need; as you get more conditioned, you can increase it.
VO2 max will go up if you just improve zone 2; to improve it further you just add a little more intense intervals. If you can walk on a 3-5% incline at 3mph, add 5 min bursts at 10% for example.
Treadmills, stairmasters, cycling all fine for cardio— you ideally want to do it with your hands off any bars supporting yourself; swimming is excellent for VO2 max
Strength
Bodyweight exercises, complex movements vs only machines - machines are still useful because they limit range of movement
Only do machines for strength training to start if they’ve never done strength training before. Machines are useful because they limit the range of movement.
Bodyweight exercises are also great to start with.
For dumbells, would only use initially for farmer’s carry.
Can push frequency first, then duration, lastly intensity. Injury usually comes from pushing intensity too quickly. Control is critical.
Make sure you eat enough protein.
There is also an extremely strong correlation between increased grip strength and decreased prevalence of Alzheimer’s disease. I think this has less to do specifically with grip strength, and more that grip strength is an easy indicator of overall strength—people who spend a lot of time lifting weights naturally build up grip strength from holding barbells and dumbbells. But it’s much easier to measure grip strength than, say, deadlifting capacity in the general population. So this is not intended as a prescription to go and buy those grip strength trainers; if you get strong overall, grip strength will follow.
Nutrition is hard to test for a few reasons. Most effects are small, making it difficult to separate correlation and causation. Attia gives an example of a study on how eating red meats leads to colon cancer. The results show that it raises risk by 17%; in comparison, smoking cigarettes puts you at 1000-2500% greater risk for lung cancer. Very few published epidemiological studies show a risk increase of even 50% for a given food. The raw data is also often not great—many nutritional studies are based on food frequency questionnaires that ask people to remember what they ate over the last month in detail. I have no idea what I ate three days ago.
I am ~150 pounds or close to 70kg. At a 3.7g/kg limit, that is 259g of protein a day, or ~835g of chicken breast, or about 1.84 pounds. Of chicken alone. Every day.